|
Conversations with Neil’s Brain The Neural Nature of Thought & Language Copyright 1994 by William H. Calvin and George A. Ojemann. You may download this for personal reading but may not redistribute or archive without permission (exception: teachers should feel free to print out a chapter and photocopy it for students). William H. Calvin, Ph.D., is a neurophysiologist on the faculty of the Department of Psychiatry and Behavioral Sciences, University of Washington. George A. Ojemann, M.D., is a neurosurgeon and neurophysiologist on the faculty of the Department of Neurological Surgery, University of Washington. |
|
Seeing the Brain Speak THE ATRIUM WAS SUNNY when I found Neil waiting for me the next week, memory on his mind. The decision on operating still hadn’t been made, and Neil was impatient. He’d taken the summer off from work to get his seizure problem fixed and, at the same time, read up on brains. But it was halfway through the summer, and still no date had been set for an operation. Indeed, I knew, George had some reservations about whether to operate at all. “George sure worries a lot about memory with these temporal lobe operations,” Neil said. “I guess finding out about my memory was really the main reason for the Wada test, that making sure my language was on the left side wasn’t the crucial issue.” That’s my understanding, too. “But even though I `passed’ the Wada test, George still seems to have memory concerns. What was the significance of passing the Wada test, anyway?” It’s now thought that recent memory requires one functioning temporal lobe. “But I have two.” That’s the point. The Wada test is supposed to temporarily mimic the effect of removing one temporal lobe — in your case, the left one — by briefly anesthetizing that side of the brain. If you have two working temporal lobes, then there shouldn’t be a major memory problem after removing one of them. But what if, unknown to anyone, your right temporal lobe was so badly damaged that it couldn’t support memory? Then both your seizures and memory would depend on the same temporal lobe — the left one — and taking it out would leave you with a severe memory deficit. Better not to operate at all. If your memory is okay during the brief period when the left side of the brain is inactivated by the anesthetic — and it was — then it probably will be after the operation. And especially so if your memory is poor when your right side is similarly inactivated. That would indicate that the right side is responsible for most of your memory. “How did they figure that out?” Measuring memory with the Wada test came about in the 1950s because of a couple of instructive cases studied at the Montreal Neurologic Institute, particularly by Brenda Milner and Wilder Penfield. Before that time, no one had paid much attention to a memory role for the temporal lobe, although it had been suggested as early as 1900. One of Milner’s cases has become quite famous under the patient’s initials, H.M. H.M. had portions of the inner side of both temporal lobes removed in 1953 for seizures and psychiatric symptoms. And he immediately developed a severe memory problem that has persisted to this day. Yet H.M.’s general intelligence is quite intact — his IQ measured a bit higher after the operation than before. Nearly all his problems are a matter of remembering things. The neurosurgeon who had done the operation sent H.M. to see Milner, and she documented the nature of the memory loss. They reported the case quite widely, so that no one else would surgically remove both temporal lobes. The other pivotal case was more like the problem that the Wada test addresses. That was a patient of Penfield’s who seemed to have damage to only the left temporal lobe, but after its removal for his seizures, suffered a considerable memory loss. He, too, seemed to be otherwise intact after that operation, returning to his job, but having to write everything down because he couldn’t remember things. Penfield and Milner guessed that there was damage to his other temporal lobe that wasn’t evident with the tests available in those days. And sure enough, when that patient died of a heart attack years later, the examination of his brain after death showed old damage in the remaining hippocampus, one of the structures on the inner part of the temporal lobe, and the structure many people now believe is a crucial one for memory. “But did H.M. lose all his memory for everything? There seem to be a whole lot of different types of memory. And every writer seems to subdivide memory differently and use his own terms to label the different types. I found it really confusing!” Welcome to the club. Essentially, a new label is added each time someone devises a different way of presenting new material, or testing its recall, or doing different things in between presentation and recall. What H.M. can and can’t do tells us some of the especially useful subdivisions of memory. Remember that H.M. had the inner portions of both temporal lobes removed, including the front two-thirds of the hippocampus on both sides. H.M. remembers who he is, where he went to school, where he lived years before the operation. So that type of memory is intact. “Those are long-term memories?” That’s as good a name as any. It’s a very resistant type of memory, in the sense that temporarily interfering with brain functions doesn’t seem to do much to long-term memories. They are there after recovering consciousness from a severe brain injury, or after the brain is short of oxygen or nutrients for awhile, or after seizures that interfere with brain electrical activity. And they are there after the inner surfaces of both temporal lobes are gone. “So they weren’t stored there — or at least, not exclusively in the temporal lobe. Sounds like those memories must be fixed in concrete — but somewhere else.” We call it consolidation. Long-term memories probably are fixed in some structural change in neurons, such as synapse size. But H.M. doesn’t have all his memories from before the operation. He has lost most of them for the several years preceding it, and he doesn’t seem to have made many new ones since the operation. “So one thing the temporal lobe must be good for is making new permanent memories, and that must take quite a while - days to years.” That’s okay as a first approximation, but nothing about memory is that simple. “That’s been the story of our conversations,” Neil chuckled. “Nothing about the brain is ever simple, although you keep telling me that memory matters are even worse.” Take distractions, for instance. Parents seem to know instinctively how to distract children from unpleasant things, and how that makes them less likely to recall them tomorrow. Distraction turns out to make a big difference in how well memories are stored. H.M. can still hang on to memories if he devotes all his attention to the matter. If you give him a string of six or seven numbers to remember and don’t disturb him, he’ll be able to tell you the numbers even after fifteen minutes. So that’s another type of memory that seems to be intact after losing both temporal lobes. It’s often called “working” or “immediate” memory. “Sounds like a memory for phone numbers to me. I can remember them long enough to dial them — so long as someone doesn’t ask me something in the meantime.” Although H.M. can remember the numbers if you don’t distract him, the moment you ask him to do something else for a moment, the memory of the numbers vanishes. What doesn’t work in H.M. is a “recent” or “short-term” memory that is “post-distractional”. That is, the defect is evident only when something has to be stored over a distraction, and it isn’t evident if the memory can be continually rehearsed without distraction. “That explains why the memory test I had to do during that Wada test was constructed the way it was. I named an object, then read a sentence, and then when the neuropsychologist yelled, `What was it?’ I was to tell him the name of the object that I had to keep in memory while I read the sentence.” That sentence serves as the distractor, to make it a test of post-distractional memory. “Clever. I guess that test was to make sure I didn’t turn out like H.M., making my living as a subject for the neuropsychologists’ memory tests. Does post-distractional memory ever fail after anything except loss of function in both temporal lobes?” Sure. We call it concussion. Football players who are concussed during a play also demonstrate this distinction between an immediate and a post-distractional memory. When they are flat on their backs on the field, and again when being helped off, they can often tell the team physician that the play they were running was “Twenty-three Tango” — and be correct. You initially think that their memory is okay. But within a few minutes, the player has no recollection of those events. Both immediate and short-term memories are pretty labile and easily disturbed by such things as a concussion. Or a shortage of oxygen in the brain, or anything like a seizure that interferes with the ongoing brain electrical activity. But the post-distractional recent memory seems to be the most labile and easily disturbed of all, and it’s the one that seems to slip away with aging. “So are there two memory defects when both temporal lobes don’t work? One for your post-distractional memory and the other for making new long-term memories?” Probably not, only one for post-distractional recent memory. It just seems as if new long-term memories have to first survive post-distractional recent memory first. There’s no separate path into long-term memory, only the one through short-term memory. So H.M.’s short-term memory deficit accounts for his long-term one, too. There’s also a temporary version of H.M.’s problem that strikes some people. They can’t remember what’s happened in the last hour or two: they know who they are, they probably know where they are — but they don’t know what they’re doing there, or how they got there. They’re confused, but all their reasoning ability is working except for their inability to remember what’s happened recently. Still, they can tell you what they were doing last night, or discuss local politics. Then the problem clears up later in the day and, except for having a permanent gap in their memories of an hour or so, they’re normal again. It’s called transient global amnesia. No treatment is needed — except reassurance — and many people never have another episode of it. “A little stroke?” asked Neil. Probably not. The current thinking is that it is more like migraine with much reduced blood flow — just involving a less common location, the inner faces of both temporal lobes. So short-term memory stops working well until full blood flow finally returns. “So far, at least, memory seems a lot easier than you led me to believe,” Neil said. “It seems a lot like my computer. There’s a buffer that acts as your immediate memory, such as the type-ahead buffer for the keyboard. My computer’s random access memory acts like your post-distractional memory, always being overwritten with new stuff. And then there’s my hard disk, once the information has gotten through the two previous stages, buffer and RAM. Once written to disk, the records survive even power failures.” “Although,” Neil said, amused, “I’m not sure I’d think much of a computer that took years to get things from RAM to the hard disc. But what’s so complicated about it?” |
|
CLASSIFYING MEMORY SEEMED SIMPLE, back when H.M. was first studied in the 1950s.
But then it was found that H.M. can remember some types of new information acquired after his
operation. He was taught to draw, while only being able to see his hand and the paper via a mirror. And he learned to trace a maze. Although he doesn’t do these perceptual-motor tasks quite as well as normals, he shows definite improvement, getting through the tasks more rapidly from day to day. Of course, if you ask him whether he had ever been taught these skills, he would deny it. He didn’t mostly remember the act of being taught, although he seemed to recognize the test apparatus, and he definitely maintained his skill, being able to do the tasks quickly that had once been difficult. So his post-distractional memory for some types of information, such as motor skills, is intact. But that for other types, the particular episodes of yesterday and today, is defective. Memory for motor skills is often called procedural memory. There are other types of “unconscious” memory, too. One is called priming, in which subsequent memory performance is changed by information encountered just previously. H.M. has intact priming, too. So he has more than just procedural memory intact — it’s an “implicit” unconscious memory that is intact. What he’s lost is the memory for the events of today, sometimes called declarative memory or explicit memory. “A different RAM for each type of memory,” Neil said. “That will make my computer a bit more complex. I do wish they’d settle on one name for each type of memory.” Sorry, no industry standards in the human memory field yet. But more subdivisions. Explicit memory seems to have two parts: semantic for general principles, facts and associations — the words of your vocabulary, for example. And episodic for unique, personally experienced events. H.M. has trouble with both — he hasn’t learned very much new vocabulary since his operation, for example. But other patients with temporal lobe damage seem to have much more trouble with “episodic” memories than with the semantic ones. And when Brenda Milner began to study patients who had temporal lobe removals on only one side, she found that they sometimes had subtle memory defects on her sensitive tests — and they differed, depending on whether the operation was on the right or left side. Left-side memory defects were mostly for words. Patients with right-sided removals had minor troubles with some kinds of spatial information. “Those crazy, jumbled figures they asked me to remember?” asked Neil. I think they must make those figures by photographing a pile of coat hangers on the floor. And then mixing them up and photographing them again. The folks with right temporal lobe removals have more trouble recognizing whether they’d seen the picture before. But these right side memory defects are for only some types of spatial information, not all types. And, of course, the problems are seen only after a distraction. “In all these examples, the memory seems either to be there, or not to be there. Yet I seem to have a lot of fuzzy memories, half remembrances. Do they ever test for them?” They’re one of the first things discovered about the psychology of memory. The nineteenth-century German psychologist Hermann Ebbinghaus memorized lists made up of three-consonant combinations that weren’t meaningful words. Then, sometime later, he retested himself and found that he retained few if any of the three-letter combinations — but he relearned the list faster than he had the first time. That suggested that something remained in his head, even if he couldn’t recall it. “Just like I relearned Spanish pretty quickly a few years ago, when we first started doing business in Latin America. And before I started taking lessons, I didn’t remember any Spanish words — even though I spoke Spanish in first grade when I had a lot of Hispanic classmates. My instructor said it’s pretty common for students like me to relearn it quickly. So some of my Spanish was there all along, but I couldn’t make use of it until my refresher course.” What you are “conscious of” may be just the tip of the iceberg. There are other unconscious memory effects, too. One memory may inhibit a second memory. Proactive inhibition is when, in trying to recall a person’s new phone number, the old number gets in the way. Retroactive inhibition is when, in trying to recall the old number, you keep getting the new one instead. “Sort of the way I’ll see someone across the room,” Neil observed, “and tell myself that it’s Jane Doe. And then realize that it really isn’t Jane Doe but someone else I know. But I can’t come up with Betty Smith’s name because Jane Doe’s name keeps getting in my way.” Until a half hour later, when Jane Doe’s name has faded and the right name finally pops to mind, unbidden. “Exactly. With all these interactions, I’m surprised anybody remembers anything with any accuracy.” |
|
OUR MEMORIES AREN’T AS RELIABLE as we’d like to think. The problem is
especially serious for an episodic memory, which is a unique category that ties together a series
of elements. Everyone thinks that recall is especially good for “flashbulb memories,” like the Kennedy assassination, but it isn’t. The morning after the disastrous explosion of the space shuttle Challenger in 1986, the psychologist Ulric Neisser asked the students in his freshman psychology class to fill out a questionnaire asking where they were when they heard the news, what they were doing at the time, who they were with, and who first told them the news. He then filed them away for three years and contacted the students when they were seniors, got them to answer the same questions again — with one additional question, asking them how sure they were of their answers. At least a quarter of the students were completely wrong in every major detail. Only about one in ten remembered the events the same as on the morning after. “They were the ones who were pretty sure of themselves?” Being positive that you’re right isn’t, alas, very reliable. The students who got things wrong in every major detail were just as likely to be confident of the accuracy of their recall. They were quite puzzled when shown the original questionnaire — in their own handwriting, furthermore. |
|
SEQUENTIAL EPISODIC MEMORIES seem to be the hardest to correctly recall. You have to
remember not only a certain set of elements, such as the who-where-what of the space shuttle
explosion news, but also the order of the elements. Sometimes, as in the case of remembering lunch yesterday, we have a mental script that helps us: it’s like a “lunch form” to be filled out. The only three mandatory items about lunch are where, when, and what — and some of those may be standard. But there are optional boxes for the common additional elements: with whom and conversation topic. Other episodes may not have this crutch, and often there is no standard script for the conversations we may experience in the course of a morning. The most common error, in real life as well as after brain injury, is to get the elements a little out of order. We might try to report accurately who said what at a particular committee meeting, but unless we have taken notes, the order of speakers is likely to become jumbled. “Eyewitnesses to a car accident are supposed to be especially unreliable,” nodded Neil. Yes, but that’s for an additional reason. Episodic memories also turn out to be easily changed afterwards, not remaining permanent as in a recording. A lot of experiments have been done by psychologists on that very topic, usually using undergraduates as research subjects. For example, Elizabeth Loftus and her colleagues staged a fake accident and videotaped it — just a simple matter of a car slowly turning a corner and bumping into a pedestrian. There were several other cars in the picture, and several other people. There was a stop sign visible. The experimenters show this tape to the subject, followed by a short quiz. During the weeks that follow, the subject is again asked questions about the videotaped episode. How many vehicles, how many people, and so forth. But there were also some misleading questions that incorporate a passing reference to a nonexistent yield sign, such as “Did another car pass the red Datsun while it was stopped at the yield sign?” The next time that he is asked what he originally saw, the answers favor the yield sign — even though it was really a stop sign. About 80 percent of normal subjects make this error. And this happens the next week as well, even without any additional misleading information, even with warnings that some misleading information was introduced. More than 90 percent of these subjects correctly identified it as a stop sign just after the original videotape viewing. But that correct memory is no longer recalled. “Ouch! It makes me worry, all those leading questions with hidden assumptions that detectives like to ask suspects. And about the lawyers rehearsing witnesses before a trial.” Maybe the original information is overwritten, maybe it’s only hard to access with that misleading information more accessible — the retrograde inhibition effect. I think that we tend, just like the football player with the concussion, to fit together the elements of the story into a reasonable order. Sometimes there is a standard lunchlike script to help us. We usually get the right elements, and often in the right order. But the person with amnesia has a more difficult time getting the right elements; they may substitute yesterday’s lunch for today’s, and they often scramble the order. Yet they seem sure of it. They’re not consciously lying, so we tend to call this confabulation. In our nighttime dreams, elements and order are really scrambled but may seem quite real to us at the time, just as a delusion does to the psychotic patient. |
|
WHERE IN THE BRAIN do memories reside? As Neil observed, with all the different types of
memory, a lot of different brain areas must be involved. He couldn’t believe it was just a
matter of the temporal lobe, or only a part of it like the hippocampus. Too big a job for one
structure, he said as we walked around the campus in the summer sunshine, carrying our coffee
cups. Right. There are different places involved, more subdivisions to learn. “I’m not sure I want to know any more divisions of memory,” Neil groaned. Suppose that I ask you to silently recall some facts from history, say of the American Revolution. That seems to activate the cerebral cortex in the parietal lobes more than in the frontal lobes. But if I ask you to silently recall an episode from childhood, perhaps a vacation trip, that will instead increase the activity of frontal lobe. Events in which you were a participant are part of episodic memories, but things you’ve learned more generally are part of semantic memories, just as vocabulary is. But the big subdivisions aren’t places in the brain. They’re the different parts of the memory process. There is a difference between memory acquisition (sometimes called encoding), memory storage, and memory retrieval. Probably the easiest way to illustrate the relationships between different brain areas and these different aspects of memory is to describe some of George’s stimulation mapping studies. George used a memory test like the one during the Wada test, which I also mentioned back when we discussed stimulating the thalamus. It’s a measure of — let’s see if I can remember all the qualifiers — post-distractional, recent, explicit, episodic memory. It’s that test which uses sets of three slides. The first just shows the object to be named. Then there is a distractor slide, a sentence to read during which the memory of the object name must be stored. Finally there’s a retrieval slide, a cue for the subject to recall the name of the object in the first slide. Sometimes George stimulates the brain during the first slide as the memory is being acquired, sometimes during the distraction slide, and sometimes during the recall attempt. But he’s always looking at how well the object name is retrieved from memory. 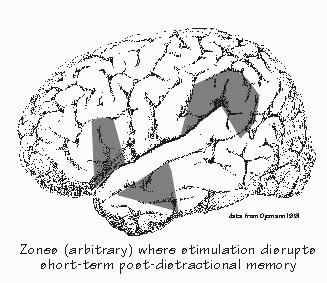 [FIGURE 41 Short-term post-distractional memory sites] The first thing he found was that this memory performance is altered from different cortical sites than the naming sites. “So if the naming sites are semantic memory,” observed Neil, “maybe these other sites store episodic memories?” Perhaps. The next thing George found was that stimulating temporal lobe sites tended to interfere with memory most when applied during the first or second slide — during acquisition and storage. Stimulating during retrieval didn’t much affect performance. By contrast, frontal lobe stimulation had effects mostly when applied during retrieval. “As if,” Neil said, “it was just distracting from the task.” Rather unexpectedly, hippocampal stimulation didn’t have much effect, unless such large currents were used that small seizures were produced on both sides. Then memory failed, regardless of whether the small seizures occurred with acquisition, storage, or retrieval. But then your memory usually fails when your seizures spread to involve the inner parts of both temporal lobes. “My seizures must be inactivating both temporal lobes,” Neil said, “as I’m temporarily like H.M. for the ten minutes or so after a seizure. I sure don’t make any new memories then. I never remember what happened during a seizure. From what you described of the stimulation studies, I’d expect memory problems with the temporal lobe, the frontal lobe, and damage down in the depths.” And that’s pretty much what we find. The most severe amnesias occur with damage to both temporal lobes, which have something to do with recent post-distractional memory storage. There’s still controversy as to exactly which structures in the temporal lobe are most critical to this process, but it’s probably both the hippocampus and the cortex. Certainly the cortex adjacent to the hippocampus is involved — in Alzheimer’s dementia, that’s where the earliest signs of neuron degeneration appear. And it probably accounts for the early symptoms of recent memory loss in Alzheimer’s. But it appears from brain-stimulation studies as if those kinds of memories also involve the evolutionarily newer parts of cortex, the ones on the side of the temporal lobe. “The cortex you see during an epilepsy operation?” Right. Much less severe memory deficits are sometimes seen after removal of the temporal lobe on only one side. As I mentioned before, you see deficits for verbal material after left removals, for spatial tasks after right removals. For example, after left temporal removals, patients may have some difficulties remembering the names of individual people or cities. “George explained to me the possibility of that type of memory loss after my operation,” Neil said, kicking a stone on the path. “But those are subtle problems compared to my seizures. So maybe I’ll have to peek in my address book more than other people do.” Memory-retrieval problems also occur with frontal lobe damage, especially when the outer part of the frontal lobe has been damaged on both the left and right sides. You see something similar in Huntington’s disease, an inherited defect in which the cells deep in the cerebral hemisphere degenerate and disrupt connections with both frontal lobes. Severe amnesias also occur with damage to subcortical structures on both sides — such as the mammillary bodies of the hypothalamus. That’s a typical location of the damage seen in Korsakoff’s syndrome, which appears in alcoholics who have a thiamine deficiency in the diet — which may be largely liquid. They have major problems in forming new memories, as well as some difficulty with retrieving previously formed long-term memories. These are the patients who usually give medical students their first experience with confabulation. “You’d think that they’d add vitamins to cheap wine,” Neil said, “just the same way as they add vitamins to milk. Wouldn’t that prevent many cases of Korsakoff’s?” Of course. Getting enough knowledge to act effectively is hard enough. Getting people to care — enough to bother doing something — seems to be the real obstacle. There are a lot of preventive measures that would reduce the number of severe mental problems. Just look at how long it took to get seat belts routinely installed in new cars, despite what everyone knew about how devastating head injuries are. And then think about how it took another quarter-century to get even half the drivers to wear their seat belts. INSTRUCTORS: You may create hypertext links to glossary items in THE CEREBRAL CODE if teaching from Chapters 6-8, e.g., <a href=http://www.williamcalvin.com/bk9gloss.html#postsynaptic>Postsynaptic</a> |
 Conversations with Neil's Brain:
Conversations with Neil's Brain: The Neural Nature of Thought and Language (Addison-Wesley, 1994), co-authored with my neurosurgeon colleague, George Ojemann. It's a tour of the human cerebral cortex, conducted from the operating room, and has been on the New Scientist bestseller list of science books. It is suitable for biology and cognitive neuroscience supplementary reading lists. ISBN 0-201-48337-8. | AVAILABILITY widespread (softcover, US$12).
|