|
Conversations with Neil’s Brain The Neural Nature of Thought & Language Copyright 1994 by William H. Calvin and George A. Ojemann. You may download this for personal reading but may not redistribute or archive without permission (exception: teachers should feel free to print out a chapter and photocopy it for students). William H. Calvin, Ph.D., is a neurophysiologist on the faculty of the Department of Psychiatry and Behavioral Sciences, University of Washington. George A. Ojemann, M.D., is a neurosurgeon and neurophysiologist on the faculty of the Department of Neurological Surgery, University of Washington. |
|
What's Up Front?
THE ROUND-THE-CLOCK EEG monitoring had resolved George’s doubts about
whether the frontal lobe might be contributing to the beginnings of Neil’s seizures. So
George finally made the decision to offer the temporal lobe operation to Neil, and Neil was quite
relieved — so relieved he plunged ahead in his brain reading and discovered that something
was missing. 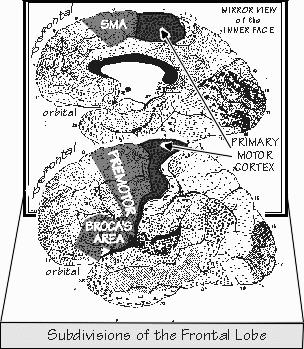 [FIGURE 46 Prefrontal, premotor, and motor subdivisions of the frontal lobe] |
|
THE FRONTAL LOBE is where forecasting-the-future abilities might be housed, since
that’s where movement planning seems to be. And the motor strip is part of the frontal
lobe, forming its rear border with the parietal lobe. Just in front of the motor strip is another “premotor” strip, all movement related. Broca’s area (or its parallel structure on the right) is at the bottom, the premotor cortex lies in the middle of the band, and the supplementary motor area starts near the top in the view from the side and continues down on the midline face of the hemisphere until stopping before the cingulate gyrus. But the functional map in this premotor strip does not parallel the head-to-hand-to-foot sequence of the motor strip. There are multiple maps of the body in this band, with the arm in front of the leg in each case. The left premotor cortex has the reputation of controlling both sides of the body to a much greater extent than the right premotor does. The premotor cortex has extensive connections to the parietal lobe and all its egocentric neurons, as well as to the thalamus (and thus the basal ganglia, another major component of the movement-control system), that the motor strip doesn’t. 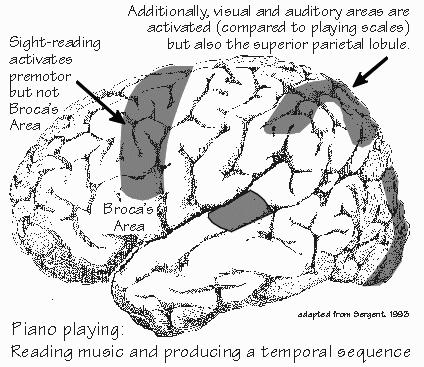 [FIGURE 47 Cortical blood flow during piano playing] When brain activity imaging is done on someone who is mentally rehearsing finger movements (but not actually moving), the supplementary motor area appears to work harder than the rest of the brain. As I mentioned before, Broca’s area plays a role in holding onto telephone numbers until they can be dialed. When playing the piano (and sight-reading music), the premotor cortex (and posterior parietal) is working hard, compared to just playing scales. The neuropsychologist Alexander R. Luria discovered a number of the more subtle aspects of movement planning when dealing with Soviet soldiers injured during the World War II. Premotor problems show up, not in individual movements like putting a key in a lock, but in sequences of actions, as when you turn the key, rotate the doorknob, and finally push open the door. Patients with damage to the left premotor cortex have trouble chaining the actions together into a fluent motion, what Luria called a kinetic melody. To tap your fingers rapidly is a typical request made by a neurologist who wants to check out premotor performance, as speed requires a lot of coordination of the movement commands. Patients with premotor problems may not be able to easily change from one rhythm to another. If asked to draw a sawtooth line but then change it to a wavy snake, the patient may be able to do each pattern separately, but not switch back and forth between patterns. The premotor cortex is all about chaining movements together, and musicians make much use of it when sight-reading, as they have to produce an unfamiliar sequence of hand and finger movements. The prefrontal cortex is in front of that premotor strip of Broca’s, premotor, and supplementary motor areas. Humans have a lot of prefrontal cortex, compared to dolphins, whose motor strip is far forward in the brain. Prefrontal cortex has a lot to do with maintaining a mental image of something in its temporary absence; monkeys with prefrontal removals will have trouble remembering where they saw their keeper hide food if they’re forced to wait more than a few minutes before being allowed out of their cage to retrieve it. Another prefrontal function noted by Luria is contingencies. Suppose that a prefrontal patient is in bed with his arms under the covers and you ask him to raise his arm. He doesn’t seem able to do so. But if you ask him to remove his arm from under the covers, he can do that. If you then ask him to raise his arm up and down in the air, he does it all correctly and smoothly. So in prefrontal problems, there is no motor-strip-like paralysis, and no difficulty with stringing together the modular movements, as the premotor cortex does for musical performance. There’s just a difficulty in planning the overall sequence, as in getting stuck on the condition of working around the obstacle of the confining bedcovers. Contingency planning, which unfolds a proper sequence of actions, is part of the role of the prefrontal cortex. At its worst, the loss of this ability after major frontal lobe damage shows up as “perseveration,” continually repeating the same action over and over again, apparently unable to shift to a new movement pattern. |
|
THE FRONTAL LOBE is about the closest thing to an executive department in the human brain.
Yet it has many reciprocal connections to the temporal lobe and the parietal lobe, big pipelines
through the white matter. They’re so extensive that a better analogy might be to the three
lobes as an executive committee. “A troika, as the Russians might say? Leaving the occipital lobe as the only part of cerebral cortex not involved in the executive?” Touché. And that’s not the only problem. Figuring out frontal lobe functions has been quite difficult. Small strokes of frontal lobe seldom come to the attention of neurologists. The symptoms are so ill defined that patients may not seek medical attention. Head injuries often produce diffuse injuries with disorderly symptoms — often these patients merely cannot plan ahead very well. Tumors of frontal lobe often grow so slowly that the functional problems are assumed to be part of aging or of a mild mental illness. One classic story is about Wilder Penfield’s sister. He operated on her for a rather large right frontal lobe tumor. Apparently she had been one of those cooks who could spend four hours preparing a five-course Christmas meal and have everything ready to come off the burner or out of the oven just when it was needed. But she lost this ability. A family dinner distressed and confused her because she could not longer get properly organized. “She couldn’t plan ahead anymore?” Or she couldn’t maintain the plan “in mind” or couldn’t monitor its progress. There’s a fascinating study of patients who had epilepsy operations on the frontal lobe because of cysts or tumors there. All the neurologists did was to ask them to count a series of clicks or taps on a finger. If they presented them at a slow rate, once per second, the patients couldn’t count them very well, but they did fine if the presentation rate was much faster. It’s totally counterintuitive. Once per second seems to require vigilance, while seven per second doesn’t. And vigilance uses the right frontal lobe, up in front of the motor strip for the left arm. Or Penfield’s sister might have had an ability to make plans but couldn’t make up her mind about which alternative was best. The neurologists talk about an accountant with a large tumor involving the base of his frontal lobes. Six years after the operation that removed the tumor, this guy exhibited a high IQ and did quite well on a battery of neuropsychological tests. Yet he had big problems in organizing his life — got fired from a series of jobs, went bankrupt, had two divorces in two years. He was often unable to make simple, rapid decisions about what toothpaste to buy or what to wear. He would instead become stuck making endless comparisons and contrasts, often making no decision at all or a purely random one. Relatively simple decisions could take hours. Going out for dinner required that he consider the seating plan, menu, atmosphere, and management of each possible restaurant. He’d even drive by them to see how busy they were, yet continue to be indecisive, unable to come to a decision about where to eat dinner. “He sounds compulsive. Like those people who keep washing their hands over and over. Compulsive contemplation.” That same region his tumor damaged — the base of both frontal lobes — sometimes lights up in the brain imaging of the people with obsessive-compulsive disorder, although other evidence suggests that their trouble may lie primarily in the basal ganglia. “So what’s the difference between obsessions and compulsions?” Thoughts versus actions — it’s probably all the same disorder, but the splitters won out over the lumpers. The common obsessions are recurrent, persistent thoughts that seem intrusive and senseless, such as excessive concern over dirt, germs, and toxins. Or thinking that something terrible is about to happen. Or perhaps an obsession with symmetry, order, or exactness. The compulsions are repetitive, purposeful behaviors that the person knows are really not necessary — such as rechecking to see that the door is locked when you’ve just done it ten minutes earlier, and ten minutes before that as well. Sometimes compulsions are in response to an obsession, sometimes they just seem to be a preoccupation with rules — such as counting to four, over and over again. And we’re now starting to recognize some minor compulsive symptoms, such as in patients who are constantly combing their hair. Fortunately, three of the many antidepressant drugs turn out to be effective for many of those people (they even work for some pets that constantly lick themselves). The effective drugs differ from the antidepressants that are ineffective for obsessive-compulsive disorder in only minor ways, sometimes just a single atom in the whole molecule. “I don’t think I’ve ever met a full-blown compulsive. Although we’re always kidding our accountant, it doesn’t sound like he’s going to qualify. He knows that it’s necessary to go through the figures three times, because he’s often found errors the second or third time through. Nothing unnecessary about it.” Right. These patients know its unnecessary — they have insight. The obsessive-compulsives seem to be rare, but that’s because they are so secretive — many of them lead secluded lives and never even seek medical help. It now looks as if they are several percent of the population, even more common than epileptics or schizophrenics. With an effective drug treatment available, perhaps more of them will venture out of seclusion. |
|
ADAPTING TO A CHANGING ENVIRONMENT is an everyday problem. Individually, we
have to adapt to changed circumstances, such as taking the bus if we can’t find a taxi. The
frontal lobe has a lot to do with developing strategies for various contingencies, with monitoring
the progress of things, and switching to an alternative tactic when necessary. “Left frontal lobe, right, or both?” Both. And for a long time, we thought that both frontal lobes had to be damaged before any symptoms occurred. We now know that damage to only one frontal lobe can be detected by certain sensitive neuropsychological tests. One is called the Wisconsin card-sorting task, which requires the patient to sort a special deck of cards into two piles. “I had that one. All cards with red symbols were supposed to be placed in the right-hand pile, all other colors in the left-hand pile.” But of course the patient has to figure this out from the responses elicited from the neuropsychologist. The patient is not given any specific instruction. He just starts sorting the cards into two piles and the neuropsychologist says yes or no after each card, depending on whether the correct criterion for sorting was used — in the example, yes if a card with a red symbol was placed on the right pile. Patients catch on to the criterion after a short while and soon are hearing a yes after each card. But that’s not the hard part. Partway through the deck, the neuropsychologist changes the criterion without any warning. Now it’s yes if cards with three symbols are placed on the right pile, regardless of color. Since the neuropsychologist doesn’t mention that the criterion has changed, the patient’s only clue is hearing no. Over and over. A normal person soon realizes that the rules have changed and tries another sorting pattern and eventually discovers the new criterion by a string of yes responses. “So that’s what was going on. It was rather fun, actually. But maybe that’s because I caught on each time she changed signals on me.” The patient with damage to one frontal lobe catches on to the original sorting strategy and gets the string of yes answers. But, when the needed strategy changes, he keeps on sorting the cards the way he started out, red on right, despite the string of no answers that this elicits. He seems unable to adapt his behavior to the new game. So it’s the same problem as in Luria’s patients, an inability to adapt behavior to contingencies. “So I guess I passed the test.” With more extensive damage the ability to abstract is lost. Neurologists often test this by asking patients to explain proverbs: “What does it mean when I say, `People who live in glass houses shouldn’t throw stones’?” After frontal damage, the patient may just paraphrase the proverb. With more extensive damage he will just repeat the proverb — one example of what is called concrete thinking. As frontal lobe function deteriorates further, the patient repeats actions over and over. We call that perseveration. And ultimately, he may become an akinetic mute, just sitting there awake, but not doing or saying anything. “Sounds like a little problem in those selective attention circuits you told me about, a while back.” Certainly this frontal lobe role in adaptive behavior is linked to the mechanisms of selective attention. The interaction back and forth between frontal cortex and thalamus selects from those sensations that are germane to the individual’s present situation and plans. Thalamic activity increases the probability that the significant sensory cues will be retained in memory, becoming part of “conscious experience.” Failure in this frontal-thalamic link accounts for loss of interest in the surroundings after frontal lobe damage. The inner and under surfaces of the frontal lobe seem to be particularly important to this link; extensive damage there is most likely to lead to that akinetic mute state. “Sounds like depression to me. But when I’m depressed, it’s not lack of interest, but a black pit, a real emotional change that I can’t seem to control. Is that frontal lobe?” One PET study showed decreased metabolic activity in the frontal lobes during depression, particularly in the left one, but whether that’s cause or effect isn’t known. Patients with frontal lobe damage also show a reduction in emotional responsiveness. George tells the story of a patient named Tom with a large tumor pressing on the inner sides of both frontal lobes. Not only had he lost interest in his former activities and surroundings and had signs of concrete thinking and perseveration, but he had lost much of his emotional responsiveness. He didn’t care about the effects of his behavior on his surroundings or on the people about him. Nor did he show any emotion when George told him about the tumor and that he’d need a major operation. Fortunately, George says the operation went well, with the tumor completely removed. Tom is apparently back to his old self now, including showing emotions. “What about sociopaths? They sure show little concern over how much they distress others.” Ah, yes — what in the nineteenth century was called “moral insanity.” They’re now called the people with antisocial personality disorder — but sociopathic personality and psychopathic personality are still common names. They’re estimated to include about 3-5 percent of men and 1 percent of women — and that’s by a definition that requires that the behaviors have been present in youth as well as adulthood. There are reports that some of these people don’t have the same autonomic reactions to disturbing pictures that normal people do. The areas of brain where damage alters emotional responsiveness also are concerned with visceral function: regulation of heart rate, blood pressure, respiration, digestive activity, and level of various hormones. As George likes to say, there really is a relation between emotion and butterflies in the stomach. “Gut feelings?” We even know one place they’re likely to come from — which is important, because that makes it a possible site for psychosomatic diseases. This link between emotion and visceral function is present at several levels in the brain and provides a basis for identifying the most emotionally responsive parts. But the overlap of frontal lobe sites for emotion and visceral function is particularly promising because of the link to the higher cognitive processes — spinning all those what-if scenarios that contribute to anxiety, worry, and suffering. Regulation of visceral functions depends on two systems. One is called the sympathetic nervous system. It prepares the body for fight or flight, raising the heart rate and the blood pressure, making your hair stand on end — and decreasing digestive activity, since its blood flow is needed elsewhere. The parasympathetic nervous system does the reverse, preparing the body for more vegetative activities. The head offices for these two systems are located in the hypothalamus, the piece of brain immediately below the thalamus and just above the pituitary gland. The hypothalamus really is the head office for regulating visceral functions, not only through the sympathetic and parasympathetic pathways but also by regulation of hormones, through its control of the pituitary gland activity.  [FIGURE 48 Hypothalamus and the limbic system] Damaging the hypothalamus in experimental animals not only disturbs the regulation of their visceral functions, but alters their emotional responsiveness. When a small area of the outer part of the hypothalamus is destroyed, cats change from being easily handled to responding with blind rage to all contact. Cats with damage a few millimeters away, in inner parts of the hypothalamus, never show rage. They become placid and fat. There are a few patients with tumors or small strokes in the different parts of the hypothalamus who had the same types of symptoms. The hypothalamus is also a major site where electrical stimulation seems to produce quite pleasurable feelings. Given a choice of food, water, sex, and a bar to press, animals will press the stimulating bar to exhaustion. “So `mean and lean’ and `fat and happy’ might be due to what kind of hypothalamus you have. Isn’t that what’s supposed to be different in the brains of homosexuals?” There’s one report of a difference in the size of one of the clusters of nerve cells in the hypothalamus, known as AH3. In that report, male homosexuals have the cluster size that’s associated with normal females, at least in this one region. A difference in the hypothalamus would not be totally surprising, though, since it has a major role in regulation of levels of the various sex hormones throughout life. But no one knows yet whether this is cause — as everyone seems to assume — or effect. It could be the atrophy of the unused. “Well, I can see how differences in function of the hypothalamus can change a person’s emotions,” Neil said. “But isn’t the cortex the real boss when it comes to emotions?” At least the more integrated emotional behaviors — hypothalamic behaviors are pretty raw and unrefined. At the hypothalamic level, emotions of rage and pleasure are little altered by any environmental stimuli. It’s at the cortical level where that interaction between environment and emotions seems to occur. The primary areas where emotional expression and visceral functions can be altered by damage or electrical stimulation are the inner surfaces of the frontal and temporal lobes. These areas have connections with the hypothalamus; together they are called the limbic system. Extensive damage to the temporal lobe portion of the limbic system on both left and right sides can lead an animal to be more likely to respond to any environmental stimulus with rage. The same thing is seen in some patients with such bilateral damage. Damage to the frontal lobe portion of the limbic system leads to placidity and indifference — as in George’s patient, Tom. “So emotionally, the real me is in my hypothalamus and limbic cortex?” There’s more. Wide areas of cortex interact with the limbic system. The mix of emotional character and thought that results is our personality. The right temporal lobe discerns the emotional coloration of faces, and emotions are more expressed on the left side of the face. Laughing and smiling, unlike other sequential face movements, are more readily disturbed from the right brain than the left. And, of course, injuries to the temporal lobe can cause someone’s personality to change. “In what way?” On Saturday morning neurosurgery rounds, I once saw a man with a head injury. The nurses had posted a handwritten sign on the door to his room: “Do not give this patient matches!” He had been mischievously lighting matches and throwing them around the room. Nothing lethargic about this guy. He didn’t want to be in the hospital. He was bright-eyed, aggressive with the docs, teasing the nurses, and generally acting like a sailor in port, looking for a good time. If he could have walked, it would have been with a swagger — however, his leg was injured also. The next Saturday, there was another temporal lobe contusion patient. This man was meek, most hesitant in his dealings with the staff, usually averting his gaze when talking with someone — totally different from last week’s patient. I didn’t realize, until we were talking about him afterward in the hallway, that this was the very same patient I’d seen the previous week. “But which was his real personality?” The second one. His family had been rather perplexed at the fun-loving sailor. Which warned the neurosurgeons that the temporal lobe’s limbic circuits were probably getting injured by brain swelling. And that they needed to do something quickly to shrink the brain a little. That usually means giving diuretics and the like, to reduce the amount of water in the uninjured regions of the brain. You can sometimes “buy time” that way. “Good thing he didn’t walk out of the hospital. God knows what he would have gotten into.” Into a coma, most likely. And an even more serious brain injury. I have a feeling that the chief resident decided that this patient’s minor leg injury required an extra-large cast. As an anchor. The cast was certainly gone at the time of my second visit. I don’t even remember seeing bandages on the leg. Some changes in temporal lobe function may be more permanent. Patients with right temporal lobe epileptic foci are said to have personalities that are more likely to show emotional responsiveness, sexuality, concern for detail, and helplessness. These patients tend to underrate their deficiencies and overrate their abilities. “Image polishers,” observed Neil. “I can hardly wait to hear about left temporal lobe epileptics. But tell me anyway.” Patients with left temporal foci — on average, and not reliably — are said to have somewhat different personalities, at least in some studies. The patient with a left temporal lobe focus more often has a moralistic, religious, rigid, sober, self-deprecating personality, tending to emphasize the personal significance of events, and often writing down all that personal significance in great detail. Both Dostoyevsky and Rasputin are thought to be examples of the left temporal lobe personality. “That left temporal epileptic personality bit is only half right for me,” reflected Neil. “Like most averages, I suppose. Sober, yes. Self-deprecating? My wife would never believe it.” It does give rise to another one of those “I can spot a case of that from across the room” stories that doctors like to tell each another. George says he can always diagnose a left temporal focus when, at the first clinic visit, he sees a patient approaching with a thick manuscript describing all his symptoms. |
 Conversations with Neil's Brain:
Conversations with Neil's Brain: The Neural Nature of Thought and Language (Addison-Wesley, 1994), co-authored with my neurosurgeon colleague, George Ojemann. It's a tour of the human cerebral cortex, conducted from the operating room, and has been on the New Scientist bestseller list of science books. It is suitable for biology and cognitive neuroscience supplementary reading lists. ISBN 0-201-48337-8. | AVAILABILITY widespread (softcover, US$12).
|